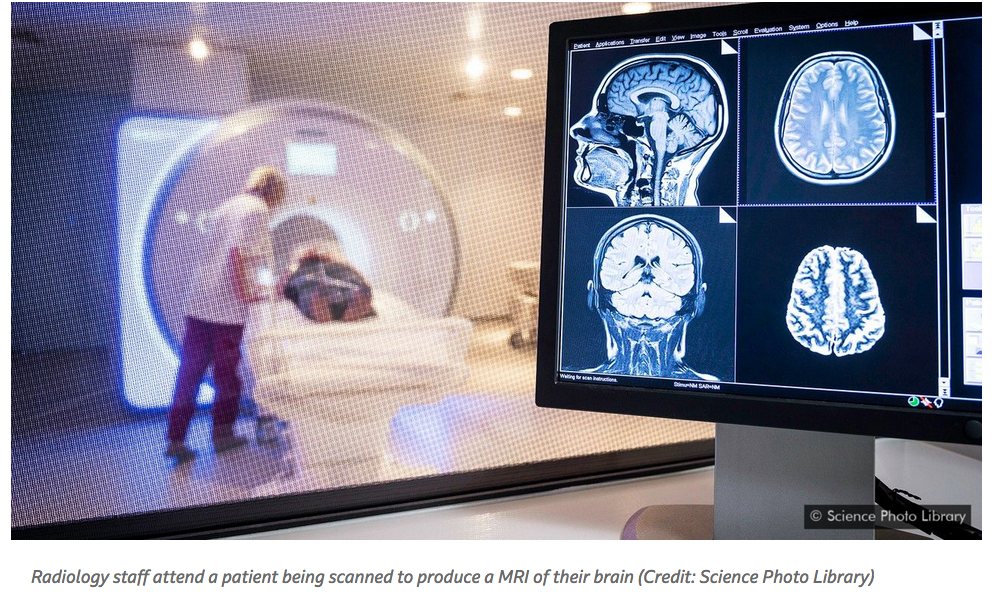
Some scientists suspect that Covid-19 causes respiratory failure and death not through damage to the lungs, but the brain – and other symptoms include headaches, strokes and seizures.

For Julie Helms, it started with a handful of patients admitted to her intensive care unit at Strasbourg University Hospital in northeast France in early March 2020. Within days, every single patient in the ICU had Covid-19 – and it was not just their breathing difficulties that alarmed her.
“They were extremely agitated, and many had neurological problems – mainly confusion and delirium,” she says. “We are used to having some patients in the ICU who are agitated and require sedation, but this was completely abnormal. It has been very scary, especially because many of the people we treated were very young – many in their 30s and 40s, even an 18-year-old.”
Helms and her colleagues published a small study in the New England Journal of Medicine documenting the neurological symptoms in their Covid-19 patients, ranging from cognitive difficulties to confusion. All are signs of “encephalopathy” (the general term for damage to the brain) – a trend that researchers in Wuhan had noticed in coronavirus patients there in February.
Now, more than 300 studies from around the world have found a prevalence of neurological abnormalities in Covid-19 patients, including mild symptoms like headaches, loss of smell (anosmia) and tingling sensations (arcoparasthesia), up to more severe outcomes such as aphasia (inability to speak), strokes and seizures. This is in addition to recent findings that the virus, which has been largely considered to be a respiratory disease, can also wreak havoc on the kidneys, liver, heart, and just about every organ system in the body.

“We don’t know yet if the encephalopathy is more severe with Covid-19 than with other viruses, but I can tell you we’ve been seeing quite a lot of it,” says neurologist Elissa Fory of the Henry Ford Foundation in Detroit, Michigan. “As the number of cases increases, you will start to see not only the common manifestations but also the uncommon manifestations – and we’re seeing them all at once, which is not something any of us have encountered in our lifetimes.”
Estimates of exact prevalence vary, but it seems that roughly 50% of patients diagnosed with Sars-CoV-2 – the virus responsible for causing the illness Covid-19 – have experienced neurological problems.
The extent and severity of these neurological issues has flown largely under the radar. Most people, including physicians, may not recognise neurological abnormalities for what they are when they appear – someone experiencing a seizure may simply look dazed, without any trembling or shaking. With its beeping machinery, sedative drugs and bed-bound isolation, an ICU environment can exacerbate and induce delirium, confounding our ability to link any symptom to the virus.
Further complicating matters, many people suffering from the effects of Sars-CoV-2 are never actually tested for the virus, especially if they do not exhibit a cough or fever. It means that if they have neurological symptoms, we may never know if this was linked to Sars-CoV-2.

“In fact, there is a significant percentage of Covid-19 patients whose only symptom is confusion” – they don’t have a cough or fatigue, says Robert Stevens, associate professor of anaesthesiology and critical care medicine at Johns Hopkins Medicine in Baltimore, Maryland.
“We are facing a secondary pandemic of neurological disease.”
A different disease
Since the start of the pandemic, it has become increasingly clear that Sars-CoV-2 is not just a turbo-charged version of the virus that causes the common cold: it has a number of quirky, unusual and sometimes terrifying traits.
For example, most viral pandemics (including influenza) have a “U shaped” mortality curve, killing the very young and the very old. But Sars-CoV-2 typically only causes mild symptoms in children. The novel coronavirus also disproportionately affects men: up to 70% of people admitted to ICUs worldwide have been male, though men and women have been infected at equal rates. (Read more about how Covid-19 affects men and women differently).

“Happy hypoxia” is another mystery. Our blood normally features “oxygen saturation” levels of around 98%. Anything below 85% should lead to a loss of consciousness, coma or even death. But a large number of Covid-19 patients have been found to have oxygen saturation levels below 70%, even below 60%, yet remained fully conscious and cognitively functional.
Then there’s the fact that an enormous percentage of people who carry the virus have no symptoms. Estimates vary, but one mass-testing report from Iceland found that fully 50% of the population who carried the virus expressed no symptoms whatsoever.
Perhaps most unnerving: while about 80% of people who develop Covid-19 shake off the virus easily, a small percentage quickly worsen and within days die from respiratory weakness and multi-system organ failure. Many of these patients are elderly or have particular underlying health conditions, but not all.
We’ve now learned that the disease affects many different organ systems: patients can die not only from lung failure, but also kidney failure, blood clots, liver abnormalities, and neurological manifestations – Robert Stevens
“If we have learned anything over the past couple of months, it is that this disease, Covid-19, is extremely heterogeneous in presentation,” says Stevens. “We’ve now learned that the disease affects many different organ systems: patients can die not only from lung failure, but also kidney failure, blood clots, liver abnormalities, and neurological manifestations.
“I’ve had patients in the ICU recover in two to three days. I’ve got others who have been in hospital now for months.”

There are other quirks that Stevens has noticed but cannot explain. “Covid-19 patients seem to have a lack of sensitivity to the drugs we normally use – we’ve had to use five to 10 times the amount of drugs for sedation that we would normally use,” he says.
Virologists will spend years trying to understand the biomechanics of this invader. And though researchers have scrutinised the virus and its victims for six months, publishing scientific studies at a rate never before seen with any disease, we still have more questions than answers. The newest to be added is: can the virus infect the brain?
Brain symptoms
Most researchers believe the neurological effect of the virus are an indirect result of either oxygen starvation to the brain (the “happy hypoxia” exhibited by many patients), or the byproduct of the body’s inflammatory response (the famed “cytokine storm”). Both Fory and Helms believe the neurological effects are “cytokine-mediated”.
Others aren’t so certain: evidence is starting to accumulate demonstrating that the virus can actually invade the brain itself.
If you had asked me a month ago if there was any published evidence that Sars-CoV-2 could cross the blood-brain barrier, I would have said no. But there are now many reports showing that it absolutely can – Stevens
“If you had asked me a month ago if there was any published evidence that Sars-CoV-2 could cross the blood-brain barrier, I would have said no – but there are now many reports showing that it absolutely can,” says Stevens.
In Japan, researchers reported the case of a 24-year-old man who was found unconscious on the floor in a pool of his own vomit. He experienced generalised seizures while being rushed to hospital. An MRI scan of his brain revealed acute signs of viral meningitis (inflammation of the brain), and a lumbar puncture detected Sars-CoV-2 in his cerebrospinal fluid. Chinese researchers also found traces of the virus in the cerebrospinal fluid of a 56-year-old male patient suffering from severe encephalitis. And in a post-mortem examination of a Covid-19 patient in Italy, researchers detected viral particlesin the endothelial cells lining the blood vessels of the brain itself. In some countries such as France, autopsies of Covid-19 patients are highly restricted (or outright banned), making the Italian finding all the more important – and concerning.
In fact, some scientists now suspect that the virus causes respiratory failure and death not through damage to the lungs but through damage to the brainstem, the command centre that ensures we continue to breathe even when unconscious.
The brain is normally shielded from infectious diseases by what is known as the “blood-brain barrier” – a lining of specialised cells inside the capillaries running through the brain and spinal cord. These block microbes and other toxic agents from infecting the brain.
If Sars-CoV-2 can cross this barrier, it suggests that not only can the virus get into the core of the central nervous system, but also that it may remain there, with the potential to return years down the line.
Though rare, this Lazarus-like behaviour is not unknown among viruses: the chickenpox virus Herpes zoster, for example, commonly infects the nerve cells in the spine, later reappearing in adulthood as shingles – roughly 30% of people who experienced chickenpox in childhood will develop shingles at some point in their lives.

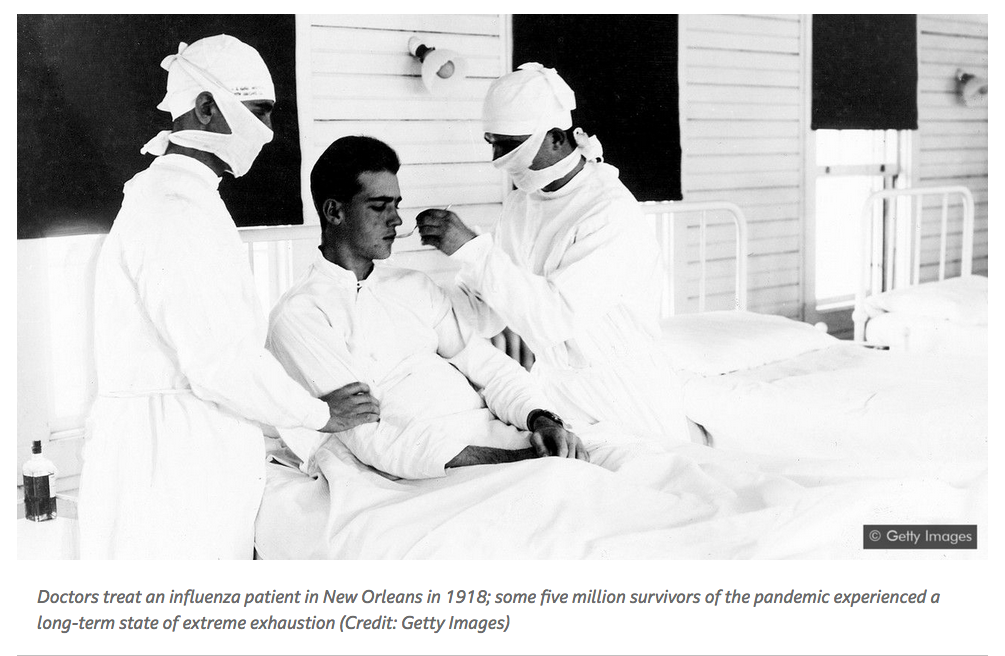
Other viruses have caused far more devastating long term impacts. One of the most notorious was the influenza virus responsible for the 1918 pandemic, which caused permanent and profound damage to the dopamine neurons of the brain and central nervous system. (While it’s long been assumed that influenza cannot cross the blood-brain barrier, some scientists now think that it can). An estimated five million people worldwide were hobbled by a form of extreme exhaustion known as “sleepy sickness” or “encephalitis lethargica”.
Among those who survived, many remained in a state of suspended animation. “They neither conveyed nor felt the feeling of life; they were as insubstantial as ghosts, and as passive as zombies,” wrote Oliver Sacks in his 1973 memoir Awakenings. He described patients remaining in this stupor for decades until being revived by the drug L-DOPA, replenishing levels of the neurotransmitter dopamine. (Read more about why the 1918 flu was so deadly).
David Nutt, professor of neuropsychopharmacology at Imperial College London, says he himself treated many patients in the 1970s and 1980s who had suffered from severe clinical depression ever since the 1957 influenza pandemic in the UK.
“Their depression was enduring and it was solid – it was if their emotional circuits had all been switched off,” he says, warning that we could see the very same thing happen again, but on a much larger scale. “People who are discharged from the ICU with Covid-19 need to be monitored systematically long-term for any evidence of neurological damage – and then given interventionist treatments if necessary.”
Patients who exhibit symptoms should be moved into interventional trials, such as of selective serotonin reuptake inhibitors (SSRI) anti-depressants or beta interferons (naturally-occurring proteins often administered as drugs for conditions such as multiple sclerosis) to mitigate the damage and prevent further long-term effects. But this simply isn’t being done, he says: “What really bugs me is that every health trust in the UK is looking at the symptoms of Covid – but nobody is looking at the neurological mechanisms, such as the amount of serotonin in the brain.”
Nutt plans to enroll 20 Covid-19 patients who developed depression or another neuro-psychiatric condition into a study that will use Imperial’s state-of-the-art PET scanners to look for signs of brain inflammation or abnormalities in neurotransmitter levels.
In Baltimore, Stevens is also planning a long-term study on Covid-19 patients discharged from the ICU, which will also conduct brain scans as well as detailed cognitive tests on functions such as memory capacity.
And in Pittsburgh, through the Global Consortium Study of Neurological Dysfunction in Covid-19, Sherry Chou, a neurologist at the University of Pittsburgh, has coordinated scientists from 17 countries to collectively monitor the neurological symptoms of the pandemic, including through brain scans.
The virus’s impact on the nervous system could be far larger and more devastating than its impact on the lungs
Although the virus’s impact on the lungs is the most immediate and terrifying threat, the lasting impact on the nervous system be far larger and far more devastating, says Chou.
“Even though neurological symptoms are less common in Covid-19 than lung problems, recovery from neurological injuries is often incomplete and can take much longer compared to other organ systems (for example, lung), and therefore result in much greater overall disability, and possibly more death,” she says.

In France, Helms knows better than almost anyone how intense the neurological impacts can be. We needed to delay her interview with the BBC after one of her Covid-19 patients – who was discharged from the hospital two months ago, but is still suffering from viral fatigue and severe depression – required urgent consultation for suicidal risk. And that patient is not unique – she has seen many people in similar states of distress.
“She is confused, she cannot walk, and she just wants to die, it’s really awful,” says Helms. “She’s only 60, but she has said to me ‘Covid has killed me’ – meaning it has killed her brain. She just doesn’t want anything more in life.
“This has been especially difficult because we don’t know how to prevent this damage in the first place. We just don’t have any treatments that will prevent any damage to the brain.”
Patients experiencing lung failure can be put on a respirator, and kidneys can be rescued with a dialysis machine – and, with some luck, both organs will bounce back. But there is no dialysis machine for the brain.